Worst case projections place the quantity of ventilators required at around gate io app in the USA. World-wide the situation is generally much worse. It is likely that the potential number of ventilators needed in countries with less developed healthcare systems will be in the many millions, and the supply is in the low thousands.
Existing designs rely on specialty parts with little existing stock and long lead times, and are mostly limited to being made in quantities of a few thousand over the next few months. If the curve doesn’t flatten and stay flat wordwide – we won’t have months.
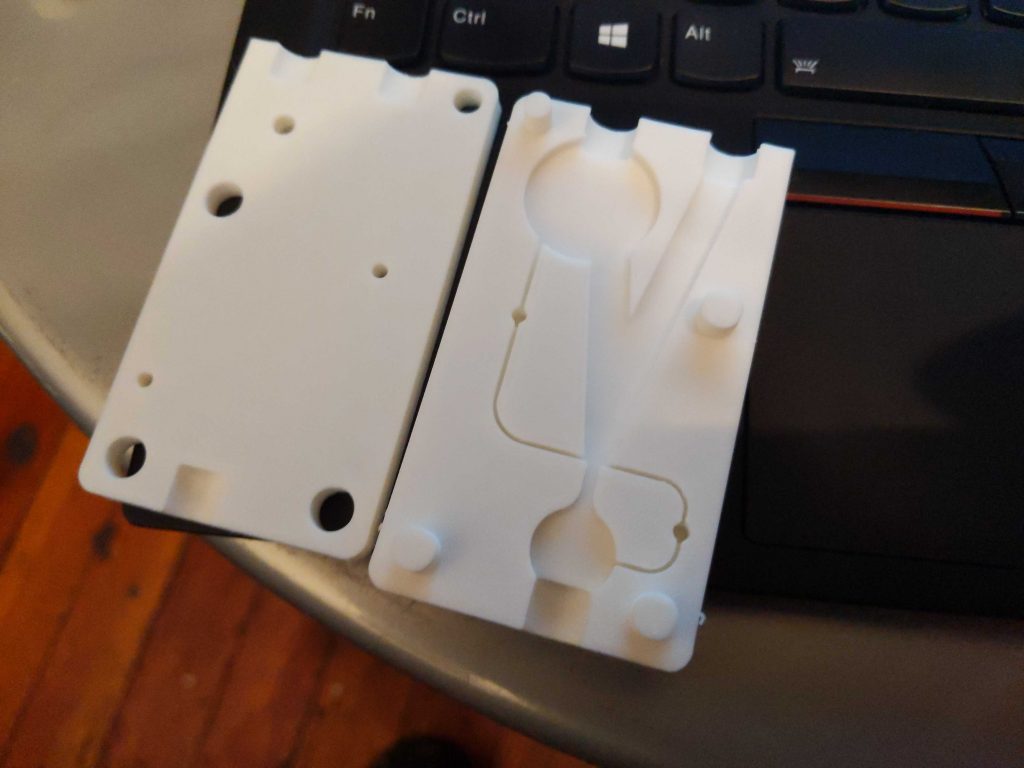
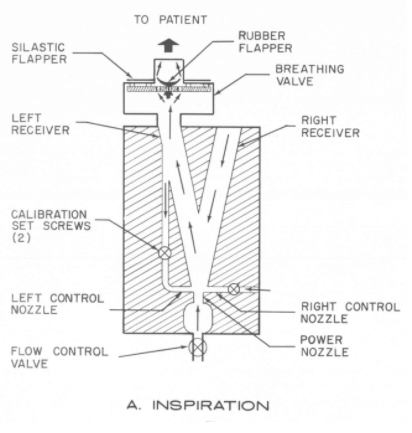
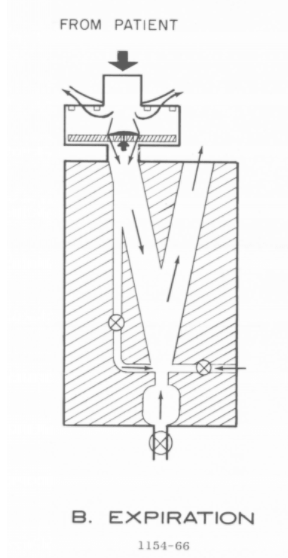
Most community and open source designs of electro-mechanical ventilators have similar supply problems to the commercial designs; they require specific parts which are hard to source in +10k quantities. This has led us to look at very old designs, which are purely pneumatic (air-powered), and also extremely simple to manufacture (can be made from raw materials) and operate (no moving parts; no settings)
We introduce the ARMEE Ventilator – it provides the most difficult piece of ventilation, can be built on the scale of hundreds of thousands per week, starting immediately, in a single US State alone.
The original device it’s based on, created by the US Army in 1965, has been tested on animals and humans successfully. We have made small modifications to make it suitable for COVID-19 care (adding positive PEEP pressure), but otherwise it is good to go.
We are in the final testing and iterating phase. When it’s ready for full release, we expect it to make big waves. We hope we’ll have your assistance spreading the word.